Call Us For Easy
Confidential Assistance
503-506-0101
It only takes 5 minutes to get started
Prescription Drug Dependency in Oregon: When to Seek Residential Treatment in the Salem Area
Posted on: April 18th, 2026 by writer

Table of Contents
- Salem’s Silent Crisis: How Prescription Drugs Have Quietly Devastated Our Community
- From Medicine Cabinet to Crisis: Recognizing the Warning Signs of Pill Addiction
- The Environmental Trap: Why Staying Home Can Sabotage Recovery
- Nature, Structure, and Science: Why Residential Treatment Works for Prescription Dependency
- Taking the First Step: How to Know When It’s Time for Residential Care
- Final Thoughts
A Salem resident picks up their prescription after shoulder surgery. The label reads “Take as needed for pain.” Six months later, they’re calling in refills early, visiting multiple doctors, and experiencing panic at the thought of running out. The medication that was supposed to heal has become a hidden prison. This scenario plays out daily across Oregon’s Willamette Valley. The numbers tell a sobering story: 5.1% of adults in the Salem region report prescription opioid misuse in the past year—higher than the state average. Even more alarming, 82% of Salem-area residents struggling with prescription dependency receive no specialty treatment whatsoever, creating a massive “treatment gap” between those who need help and those who receive it. For families watching a loved one spiral deeper into pill addiction, the question isn’t whether to seek help—it’s what kind of help will actually work. This article cuts through the confusion to help Salem-area residents understand when outpatient care isn’t enough and why residential treatment offers the highest probability of lasting recovery. You’ll discover the local scope of this crisis, learn to recognize clinical warning signs, understand why staying home often sabotages recovery, and see how immersive treatment at facilities like Pacific Ridge addresses the root causes of addiction in ways weekly therapy sessions simply cannot.
Salem’s Silent Crisis: How Prescription Drugs Have Quietly Devastated Our Community
While news headlines focus on illicit drugs, prescription medications have been quietly devastating communities throughout Oregon’s Willamette Valley. Marion County—home to Salem—reports 15.6 emergency department visits per 10,000 residents for drug overdoses, exceeding the state average of 14.2. These aren’t strangers in dark alleys; they’re our neighbors, coworkers, and family members who started with a doctor’s prescription. The prescription drug crisis in Oregon carries unique characteristics that make it particularly insidious. Unlike street drugs, prescription medications come with the perception of safety because they were once doctor-prescribed. This “legality trap” creates a dangerous blind spot where individuals rationalize continued use long after therapeutic need has ended. A Xanax prescription for temporary anxiety becomes a daily necessity. Pain pills for a sports injury transform into a chemical crutch for managing everyday stress. The gateway effect compounds the danger. Research from the Oregon Health Authority shows that prescription opioids frequently serve as a stepping stone to more dangerous synthetic opioids like fentanyl. What begins as hydrocodone for back pain can progress to illicitly obtained pills, then to substances the individual never imagined they would use.
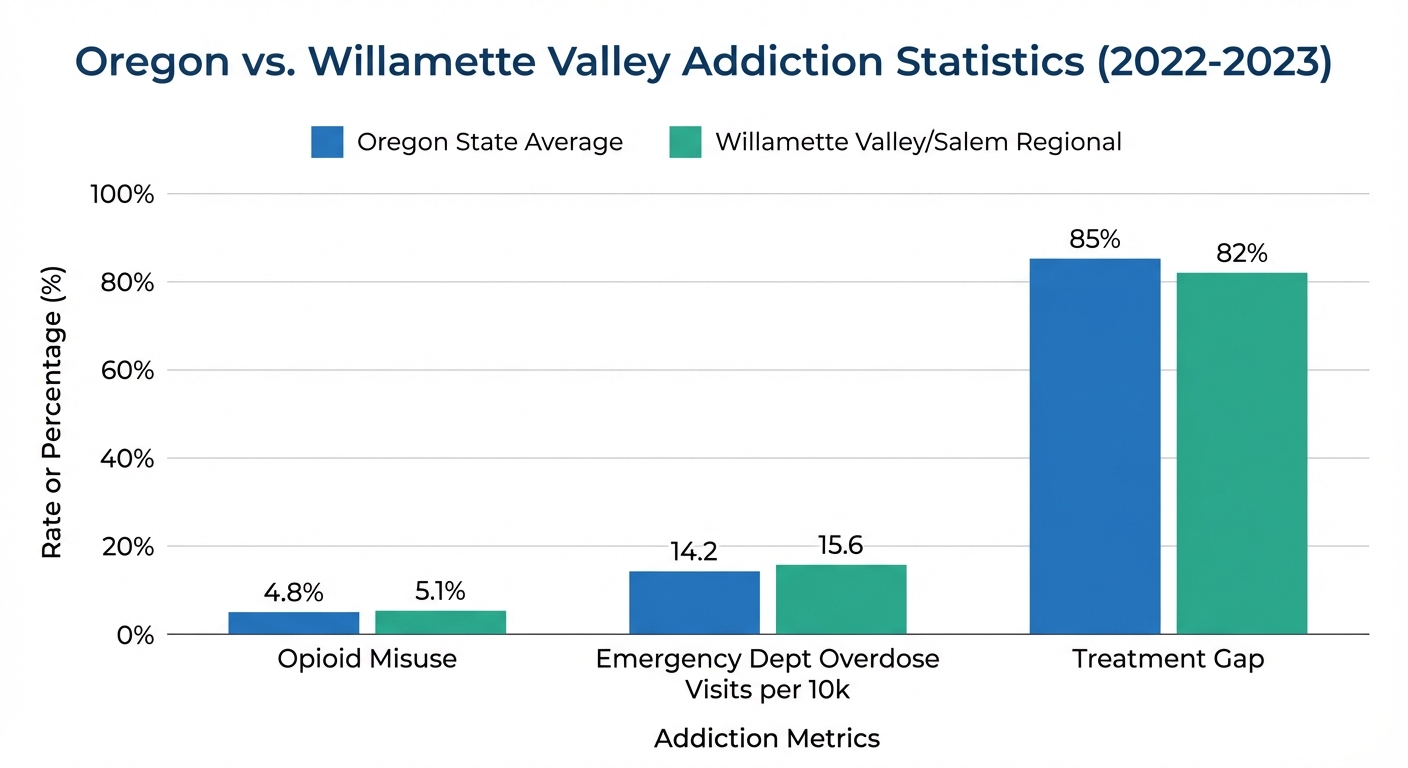
The demographic landscape of prescription dependency is also shifting in concerning ways. While chronic pain patients historically dominated cases, recent data reveals sharp increases among young adults ages 18-25 misusing prescription stimulants like Adderall and Ritalin, as well as benzodiazepines like Xanax and Valium. College students seeking academic performance enhancement, young professionals managing workplace stress, and individuals self-medicating anxiety disorders are fueling this troubling trend. The treatment gap is perhaps the most disturbing statistic: 82% of Salem-area residents with prescription dependency receive no specialty treatment. They suffer in silence, believing they should be able to “just stop” or that their situation isn’t serious enough to warrant professional help. By the time families reach out for treatment, the dependency has typically progressed from moderate to severe, requiring more intensive intervention than initially would have been necessary.
From Medicine Cabinet to Crisis: Recognizing the Warning Signs of Pill Addiction
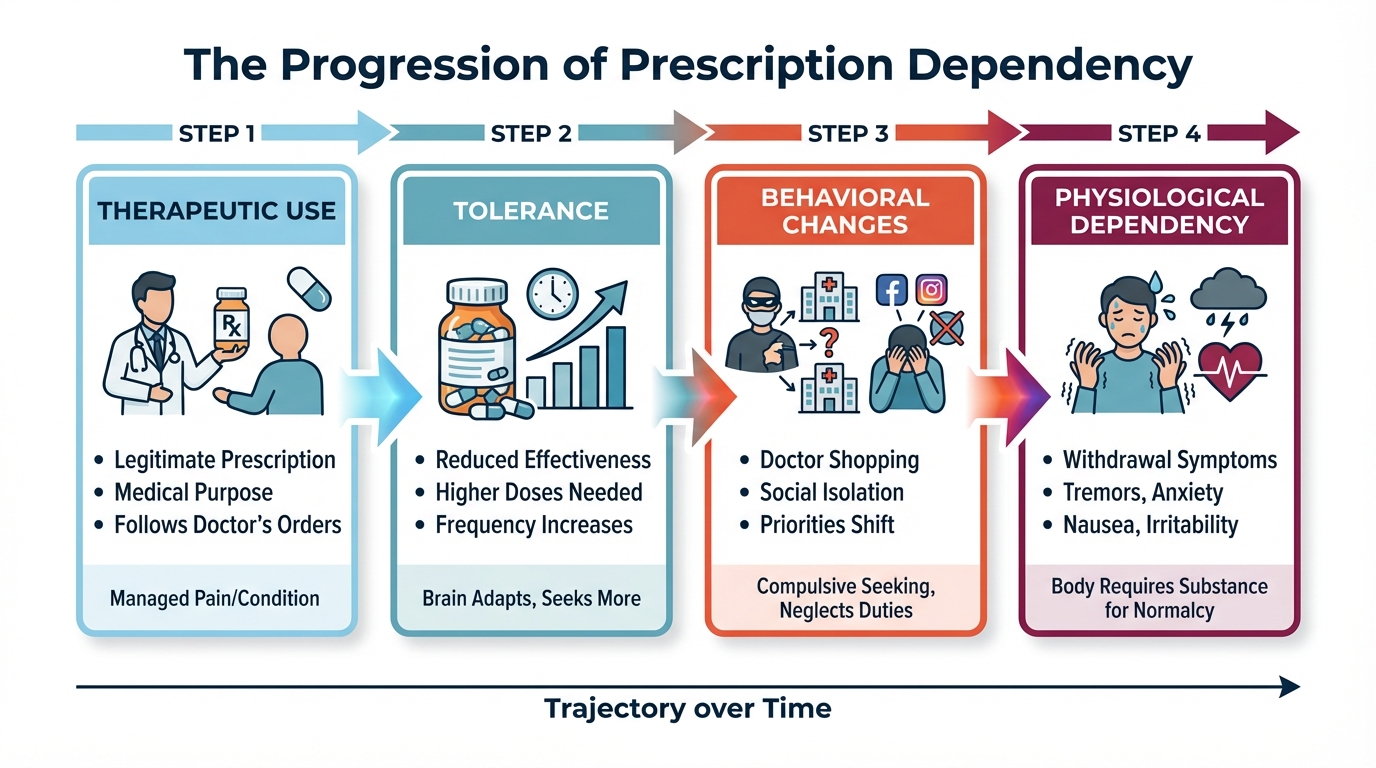
Understanding how prescription use transforms into dependency requires examining both the neurobiology of addiction and the observable warning signs that families should monitor. The National Institute on Drug Abuse defines addiction as “a chronic, relapsing disorder characterized by compulsive drug seeking despite adverse consequences”—a medical condition, not a moral failing. The progression begins with tolerance. The brain adapts to the presence of prescription drugs by adjusting neurotransmitter production and receptor sensitivity. A dose that initially provided eight hours of pain relief now barely lasts four. The Xanax that once calmed a panic attack no longer touches the anxiety. This neurological adaptation drives dose escalation, often without the individual consciously recognizing what’s happening.
Physical Warning Signs
Physical warning signs emerge as the body becomes chemically dependent. When doses are delayed or reduced, withdrawal symptoms appear:
- Tremors and excessive sweating
- Severe anxiety that feels different from the original condition
- Gastrointestinal distress
- Muscle aches and pain
- Sleep disturbances and insomnia
Many individuals interpret these symptoms as evidence they “need” the medication, not recognizing them as withdrawal. The medication that was supposed to solve a problem has created a new one.
Behavioral Red Flags
Behavioral red flags often become visible to family members before the individual acknowledges a problem. “Doctor shopping”—visiting multiple physicians or emergency rooms in Salem and surrounding communities to obtain overlapping prescriptions—represents a clear escalation. The individual may become increasingly isolated from family, friends, and activities they once enjoyed, whether that’s hiking Silver Falls, attending community events, or simply having dinner together. Defensiveness or secretiveness about medication use intensifies. Questions about prescriptions trigger anger or elaborate justifications.
Key Behavioral Changes to Watch For:
- Visiting multiple doctors or pharmacies in different Salem-area locations
- Withdrawal from previously enjoyed hobbies and social activities
- Defensive reactions when questioned about medication use
- Unexplained financial strain or requests to borrow money
Financial strain frequently accompanies behavioral changes. Insurance companies limit prescription quantities and refills, forcing individuals to pay out-of-pocket or seek pills through unofficial channels. Money that once went toward family activities or savings disappears. Unexplained cash withdrawals or requests to borrow money become more frequent.
Psychological Indicators
The psychological indicators are equally telling. Preoccupation with medication dominates thoughts: counting pills, calculating when the next dose can be taken, anxiety about running out. The individual continues use despite obvious negative consequences—job performance declines, relationships deteriorate, health problems emerge—yet stopping feels impossible. Hobbies and interests that once brought joy now seem irrelevant compared to the need to maintain the medication supply. This represents the complete takeover of the brain’s reward system, where the drug has become more important than virtually everything else in life. For Salem-area families, recognizing these warning signs early creates the opportunity for intervention before the dependency progresses to life-threatening severity. However, recognition alone isn’t enough—choosing the right level of treatment becomes the next critical decision.
The Environmental Trap: Why Staying Home Can Sabotage Recovery
When families first seek treatment for prescription dependency, outpatient programs often seem like the logical choice. The individual can maintain their job, stay connected to family, and attend therapy sessions a few times per week. On the surface, this appears less disruptive than residential treatment. Unfortunately, the evidence reveals a different reality: for moderate-to-severe prescription dependency, traditional outpatient care struggles to achieve lasting results. The fundamental problem is environmental. Outpatient care requires patients to return nightly to the exact environment where their addiction developed—the same home, the same stressors, the same routines, the same access points to medications. That medicine cabinet still contains leftover prescriptions. The pharmacy where they obtained pills is still on their daily commute. The friend who sometimes shares pills is still texting. The job stress that triggered anxiety is still present every morning. These environmental triggers constantly activate craving responses, making sustained recovery extraordinarily difficult.
The Therapy Hours Gap
Intensive Outpatient Programs (IOPs) typically provide only 3-9 hours of therapy per week. That leaves 159-165 hours each week when the individual must independently manage cravings, navigate triggers, and resist the urge to use—all while maintaining regular life responsibilities. For someone whose brain has been chemically altered by prolonged prescription drug use, this expectation is often unrealistic. The medical supervision gap presents genuine danger, particularly for individuals dependent on benzodiazepines or opioids. Prescription withdrawal can be medically serious and intensely uncomfortable. Benzodiazepine withdrawal can trigger seizures. Opioid withdrawal, while rarely life-threatening, produces symptoms so severe that most individuals relapse within days without medical support. Outpatient settings cannot provide 24/7 monitoring during these acute withdrawal phases, leaving patients to manage dangerous symptoms at home.
Critical Statistics on Outpatient Treatment Challenges:
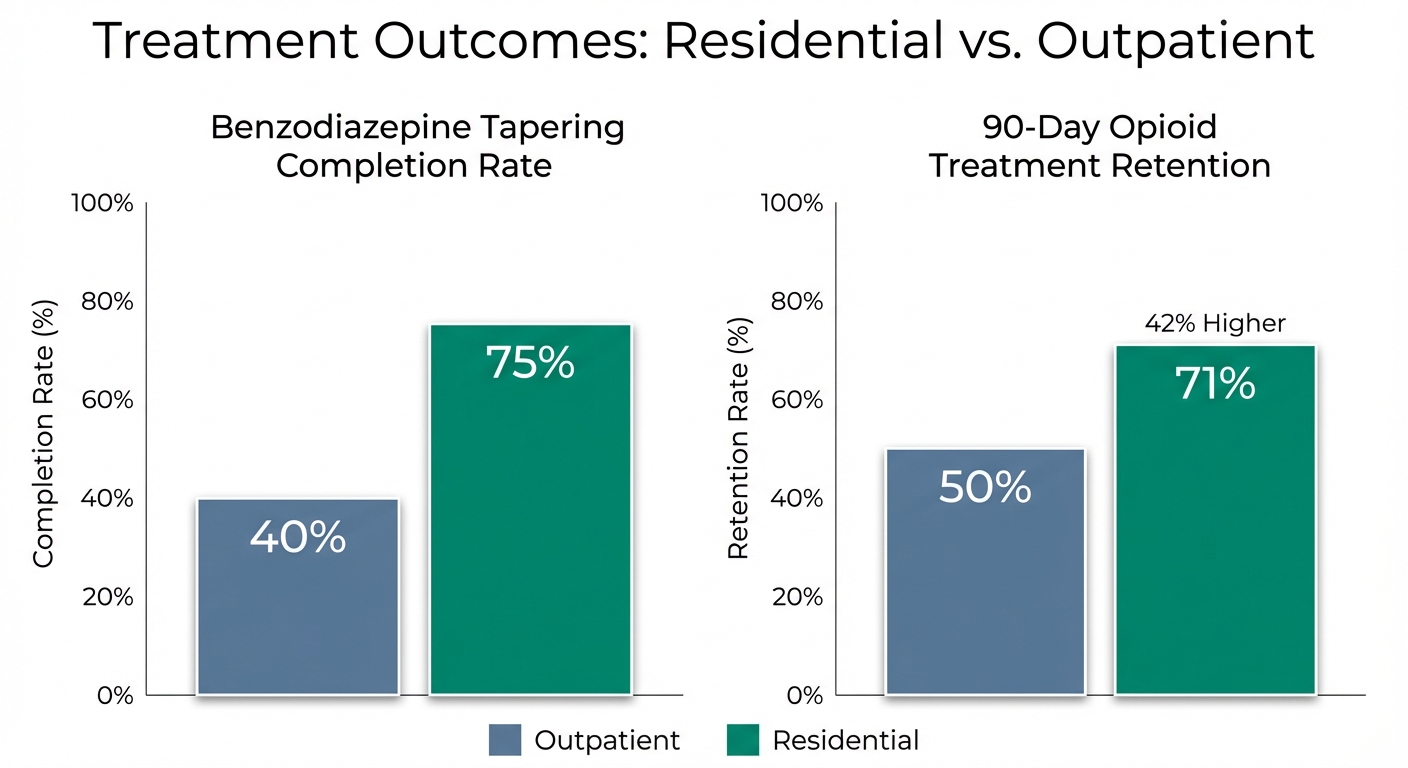
- 60% failure rate for benzodiazepine tapering in outpatient settings within the first month
- 42% higher retention rate at 90 days for residential programs compared to intensive outpatient programs
- 159-165 hours per week that patients must manage independently in outpatient care
Statistical data confirms these limitations. Research on benzodiazepine tapering shows a 60% failure rate within the first month when attempted in outpatient settings. Patients simply cannot tolerate the rebound anxiety and withdrawal symptoms without intensive medical and psychological support. A landmark study comparing treatment outcomes for opioid dependency found that residential programs demonstrated a 42% higher retention rate at 90 days compared to intensive outpatient programs. For Salem residents specifically, the daily commute to a downtown clinic for therapy creates additional relapse risks. The drive passes familiar pharmacies, potentially crosses paths with old using friends, and traverses locations associated with past drug acquisition. Each trip to treatment ironically exposes the individual to the very triggers they’re trying to overcome. The reality isn’t that outpatient programs are poorly designed or that clinicians aren’t skilled. The problem is fundamental: you cannot effectively treat an environmental disease while keeping the patient in the toxic environment. For prescription dependency that has progressed beyond the earliest stages, the environmental control offered by residential treatment becomes not just beneficial, but often essential for success.
Nature, Structure, and Science: Why Residential Treatment Works for Prescription Dependency
Residential treatment operates on a fundamentally different model than outpatient care, one supported by decades of addiction neuroscience research. The concept is called “milieu therapy”—where the environment itself becomes a therapeutic tool. An 18-acre secluded facility surrounded by Oregon’s natural beauty isn’t just pleasant aesthetics; it’s a carefully designed intervention that allows the brain to heal.
The Neurological Reset
Physical separation from drug sources and daily stressors provides the neurological “reset” that brain science shows is necessary for recovery. When an individual remains in their trigger-rich home environment, every familiar sight, sound, and routine activates the neural pathways associated with drug use. The brain continuously fires craving responses that overwhelm willpower and good intentions. Removing the individual to a completely new environment interrupts these automatic patterns, allowing the central nervous system to stabilize without constant trigger activation. Medical detoxification under 24/7 supervision addresses one of the primary reasons outpatient treatment fails. On-site medical teams can safely manage withdrawal symptoms using evidence-based pharmacotherapy, preventing dangerous complications while significantly reducing discomfort. For benzodiazepine dependency, this means a carefully calculated taper protocol that avoids seizure risk while gradually allowing the brain to readjust. For opioid dependency, it might involve medication-assisted treatment to ease withdrawal while blocking the euphoric effects of opioids.
Comprehensive Therapeutic Programming
The intensity of therapeutic programming in residential settings far exceeds what outpatient care can provide. Patients engage in 30+ hours of therapy per week, including:
- Cognitive Behavioral Therapy (CBT) to identify and change thought patterns that drive drug use
- Dialectical Behavior Therapy (DBT) to build emotional regulation skills
- Group therapy for peer support and accountability
- Recreational therapy that leverages Oregon’s natural environment for healing
This comprehensive approach addresses the psychological, emotional, behavioral, and spiritual dimensions of addiction simultaneously. Research consistently demonstrates residential treatment’s superiority for severe substance use disorders. A study published by the American Psychiatric Association found that residential programs achieve completion rates exceeding 75% for benzodiazepine tapering, compared to only 40% in outpatient settings. The difference isn’t marginal—it’s the difference between success and failure for most patients.
The Power of Peer Community
Peer community healing represents another critical advantage. Living alongside others in recovery creates natural accountability, reduces the profound isolation that accompanies addiction, and builds lifelong support networks. Shared meals, group activities, and simply existing in community with others who understand the struggle creates bonds that continue supporting recovery long after treatment ends. This stands in stark contrast to outpatient care, where individuals return home each night to isolation and must rely solely on their own resolve. For Salem-area residents, facilities like Pacific Ridge offer an additional advantage: geographical proximity that allows family involvement without requiring the individual to remain in their trigger environment. Family members can participate in family therapy sessions and educational programming, staying connected while their loved one receives world-class care in a healing setting designed specifically for recovery.
Taking the First Step: How to Know When It’s Time for Residential Care
The decision to pursue residential treatment often feels overwhelming. Families worry about work obligations, financial concerns, and whether such intensive intervention is truly necessary. Understanding when residential treatment becomes essential—rather than simply preferable—can provide clarity during a confusing time.
Critical Assessment Questions
Several assessment questions can guide this decision:
Key Questions to Consider:
Has outpatient treatment been attempted without success?
If previous outpatient programs haven’t achieved lasting results, continuing the same approach while expecting different outcomes isn’t realistic. Residential care represents the necessary escalation in treatment intensity.
Are co-occurring mental health conditions present?
Depression, anxiety disorders, PTSD, or other psychiatric conditions significantly complicate recovery from prescription dependency. Residential programs can provide integrated treatment for both addiction and mental health conditions simultaneously, something outpatient care struggles to coordinate effectively.
Is the home environment enabling or triggering continued use?
Honest assessment of the home environment is crucial. Does the individual live with others who use substances? Are there unresolved conflicts or stress sources that trigger drug use? Is the individual isolated without supportive relationships? An unsupportive home environment dramatically reduces outpatient treatment success rates.
Are there safety concerns related to withdrawal or overdose risk?
High-dose dependency, particularly on benzodiazepines or opioids, creates genuine medical dangers during withdrawal. Polysubstance use (combining multiple drugs) compounds these risks. If there’s any concern about safe withdrawal, residential treatment with 24/7 medical supervision becomes medically necessary, not just preferable.
Does the individual have a strong support system, or are they isolated?
Addiction thrives in isolation. Individuals lacking supportive relationships, stable housing, or meaningful daily structure face dramatically higher relapse rates in outpatient care. Residential treatment provides the structured community and support that’s missing from their current life.
When Residential Treatment Becomes Essential
Residential treatment becomes essential rather than optional when several conditions converge:
- High-dose or polysubstance dependency
- Previous failed outpatient attempts
- Lack of safe supportive home environment
- Medical complications requiring supervised detox
- Severe co-occurring mental health disorders
Under these circumstances, outpatient care isn’t just less effective—it’s often ineffective. For Salem-area families, an important perspective shift involves understanding that residential treatment isn’t abandonment or giving up. It’s providing the highest level of care available while creating space for both the individual and family system to heal. Family members can participate in therapeutic programming specifically designed for families, learning how to support recovery rather than inadvertently enable addiction.
Insurance and Accessibility
Insurance and accessibility concerns frequently create hesitation. Many Oregon insurance plans cover residential treatment, particularly when medical necessity can be demonstrated through previous failed treatments or co-occurring conditions. Facilities like Pacific Ridge work directly with families to navigate insurance coverage, verify benefits, and explore financial options that make treatment accessible. The geographic advantage for Salem residents shouldn’t be overlooked. Proximity to Portland and Eugene means family can visit while the individual receives comprehensive care in a healing environment. This balance—close enough for family involvement but far enough to escape daily triggers—provides optimal conditions for recovery.
Final Thoughts
Prescription drug dependency is a medical condition requiring medical intervention, not a moral failure requiring stronger willpower. The brain changes that occur during prolonged prescription drug use are real, measurable, and require professional treatment to reverse. For individuals and families in the Salem area struggling with this crisis, understanding the level of care necessary can mean the difference between continued suffering and lasting recovery. The clinical evidence is unequivocal: for moderate-to-severe prescription dependency, residential treatment offers the highest success rates for long-term recovery. By providing physical separation from environmental triggers, continuous medical supervision during withdrawal, intensive therapeutic programming, and a supportive peer community, residential facilities create conditions that allow the brain to heal in ways that simply aren’t possible while remaining in the environment where addiction developed. Marion County’s 15.6 overdose-related emergency department visits per 10,000 residents represent more than statistics—they represent Salem neighbors, family members, and community members in crisis. With 82% of individuals with prescription dependency receiving no specialty treatment, waiting isn’t a neutral choice. Addiction is progressive. What feels manageable today will likely be more severe tomorrow. Early intervention doesn’t just improve outcomes—it saves lives.
“Recovery is possible. Thousands of individuals have rebuilt their lives through immersive, residential treatment programs that address the root causes of addiction rather than simply managing symptoms.”
Recovery is possible. Thousands of individuals have rebuilt their lives through immersive, residential treatment programs that address the root causes of addiction rather than simply managing symptoms. The prescription pills that once felt like a prison can become part of a past that no longer defines the future. But that future requires taking the first step: acknowledging that outpatient care isn’t always enough and that sometimes the most powerful choice is seeking the highest level of care available.
Ready to Take the First Step Toward Recovery?
If you or someone you love in the Salem area is struggling with prescription dependency, Pacific Ridge offers evidence-based, compassionate residential treatment in a setting designed specifically for healing.
Taking the first step toward residential treatment isn’t giving up—it’s choosing to fight for your future with the best tools available.
References:
- Substance Abuse and Mental Health Services Administration (SAMHSA). (2023). National Survey on Drug Use and Health (NSDUH): State Estimates.
- Oregon Health Authority (OHA). (2024). Opioid Overdose Public Health Surveillance Dashboard.
- National Institute on Drug Abuse (NIDA). (2022). Misuse of Prescription Drugs Research Report.
- National Institute on Drug Abuse (NIDA). (2020). Principles of Drug Addiction Treatment: A Research-Based Guide (Third Edition).
- Mayo Clinic. (2023). Prescription Drug Abuse: Symptoms and Causes.
- National Center for Biotechnology Information (NCBI) / National Institutes of Health. (2014). Outcomes of Residential versus Outpatient Treatment for Opioid Use Disorder. Journal of Substance Abuse Treatment.
- American Psychiatric Association. (2019). Clinical Effectiveness of Residential Treatment vs. Outpatient Care for Severe Substance Use Disorders. Psychiatric Services Journal.
Posted in Treatment
Are you looking for help?
Pacific Ridge is a residential drug and alcohol treatment facility about an hour from Portland, Oregon, on the outskirts of Salem. We’re here to help individuals and families begin the road to recovery from addiction. Our clients receive quality care without paying the high price of a hospital. Most of our clients come from Oregon and Washington, with many coming from other states as well.
Pacific Ridge is a private alcohol and drug rehab. To be a part of our treatment program, the client must voluntarily agree to cooperate with treatment. Most intakes can be scheduled within 24-48 hours.
Pacific Ridge is a State-licensed detox and residential treatment program for both alcohol and drugs. We provide individualized treatment options, work closely with managed care organizations, and maintain contracts with most insurance companies.
Quick links
Recent Posts
Contact Us
Pacific Ridge- 1587 Pacific Ridge Ln SE
Jefferson, OR 97352 - Email:
[email protected] - Phone:
503-506-0101 - Fax:
503-581-8292
- Copyright © 2026 Pacific Ridge - All Rights Reserved. Web Design & SEO by Lithium
- Follow us on